Most weight loss surgeries are currently being done by the laparoscopic approach, and gastric bypass is not an exception. Therefore, gastric bypass scars are not expected to be different from scars of other bariatric surgeries. Rarely, gastric bypass surgery may be done using the open technique.
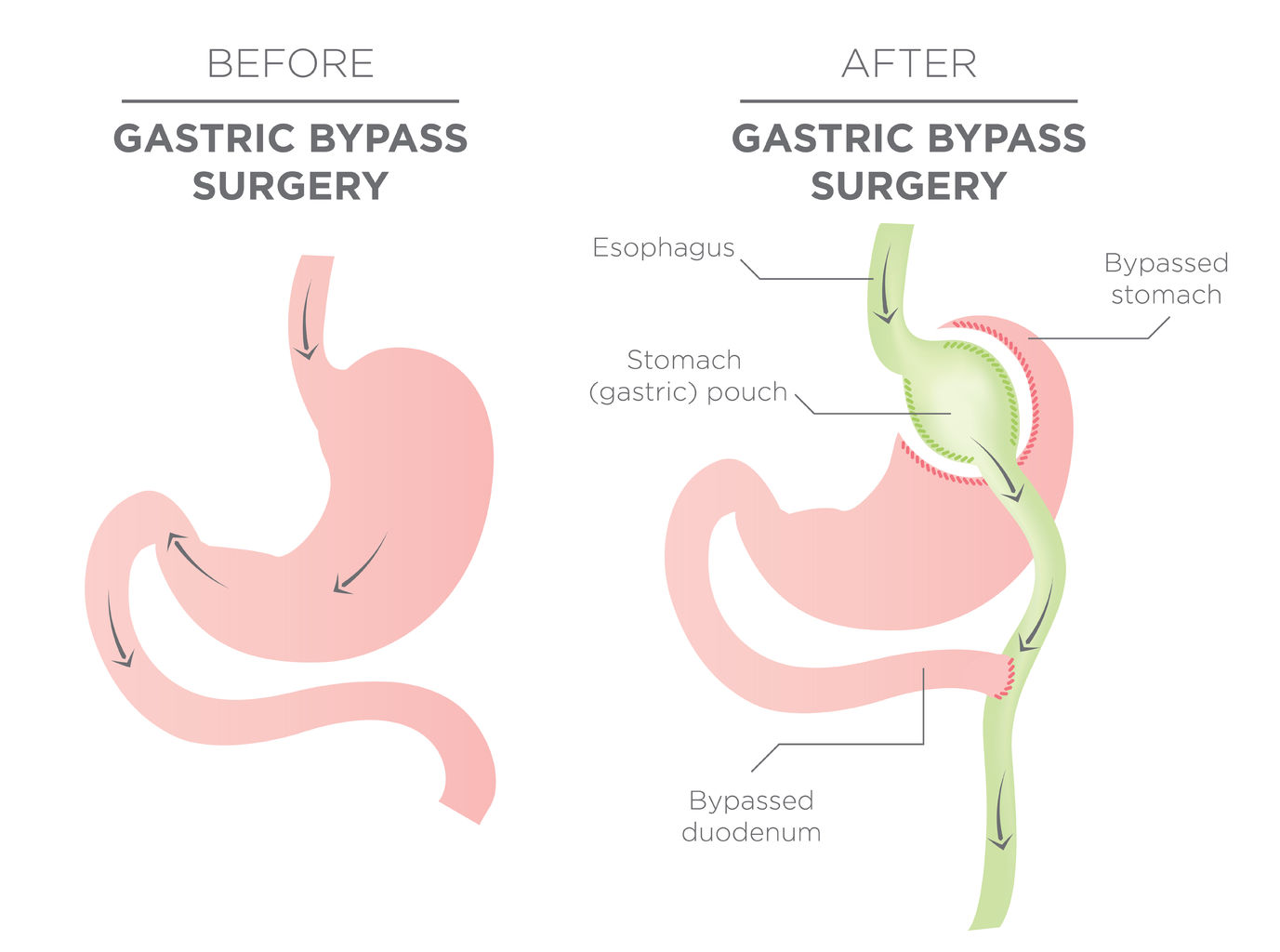
The most typical form of gastric bypass surgery is the Roux-en-Y gastric bypass. This surgery combines both restrictive and malabsorptive mechanisms. Another way of gastric bypass surgery is the mini-gastric bypass which is necessarily the same with Roux-en-Y gastric bypass in terms of mechanism of inducing weight loss but different in the terms of manipulation done on the digestive tract. They can both be done by laparoscopic or open approach.
Laparoscopic gastric bypass surgery is done by introducing some instruments (with a camera) into the abdominal cavity through a small surgical incision which is usually made around the umbilicus. In addition, about 4 similar incisions are also made on other parts of the abdominal wall for more equipment, convenience and easy manipulation. These openings are referred to as ports. The camera enables the abdominal organs and the surgical manipulations to be viewed on a monitor.
In open approach, an incision is made in the middle of the anterior abdominal wall. This may extend well above and below the umbilicus. The only advantage of this type of incision is that it gives a direct view of the abdominal organs but the resulting scar is cosmetically unacceptable to most patients.
It is also important to know that surgical scars differ from one patient to another. While some patients may end up with fine and less conspicuous scars, others may have hypertrophic (raised) and ugly scars. Some factors such as skills of the surgeon, type, and size of suture materials, genetic characteristics of the patient (e.g., keloid formers) and wound infection may also affect the final appearance of the scar.
For laparoscopic gastric bypass surgery, the final scars are about 5 in number. Each of them is less than 1cm in diameter. The one around the umbilicus is usually not obvious and with time tends to blend with the umbilicus. The other scars, after many years, may become inconspicuous as well and only identified by relatively dark skin at the sites. Thus, scars of laparoscopic gastric bypass surgery are often cosmetically acceptable to most patients.
Following open gastric bypass surgery, the abdominal wound takes a longer time to heal and is more prone to infection. The scar is usually a vertical one extending above and below the umbilicus and typically noticeable. It may be raised in some individuals.
How to have beautiful and less apparent scars
Making incisions along the line of skin crease will result in a less noticeable injury. Ensuring that the wound is not closed under tension will also prevent wound breakdown which may lead to healing with fibrosis and subsequently raised scar. You should, therefore, choose an experienced surgeon for your gastric bypass surgery.
Prevention of wound infection/immediate intervention at the early stage before wound breakdown is another way of ensuring proper healing and flat scars. Report any undue pain at the wound site to your surgeon during the first postoperative period for immediate intervention.
Go for laparoscopic surgery unless contraindicated. Except there are health conditions that prevent you from the laparoscopic gastric bypass, open surgery shouldn’t be a preference.
In summary, gastric bypass surgery is effective bariatric surgery. It can be done through laparoscopy or by the open approach. However, the former gives the most cosmetically acceptable scars.