
Surgical treatment of obesity is currently the most effective way of achieving a significant and satisfactory weight loss with improvement in obesity-associated disease conditions. Gastric bypass is one of these surgical procedures. While there is no absolute contraindication to gastric bypass, many obese individuals prefer to go for gastric bypass alternatives such as gastric sleeve, gastric balloon or gastric banding. This preference might not be unconnected to the difference in cost, complication and side effects. A comparison of these four procedures is therefore needed to make an informed decision.
Cost
The average cost of gastric bypass is about $21,000 ($17,000-$30,000) in the United States. This is closely followed by gastric banding (Lap-Band) with a mean cost of $18,000 ($15,000 to $24,000). Gastric sleeve surgery costs $15,000 ($12,000-$20,000) and gastric balloon requires about $3,000 to $9,000 in the U.S. depending on the hospital and the type of balloon.
Mechanism of action
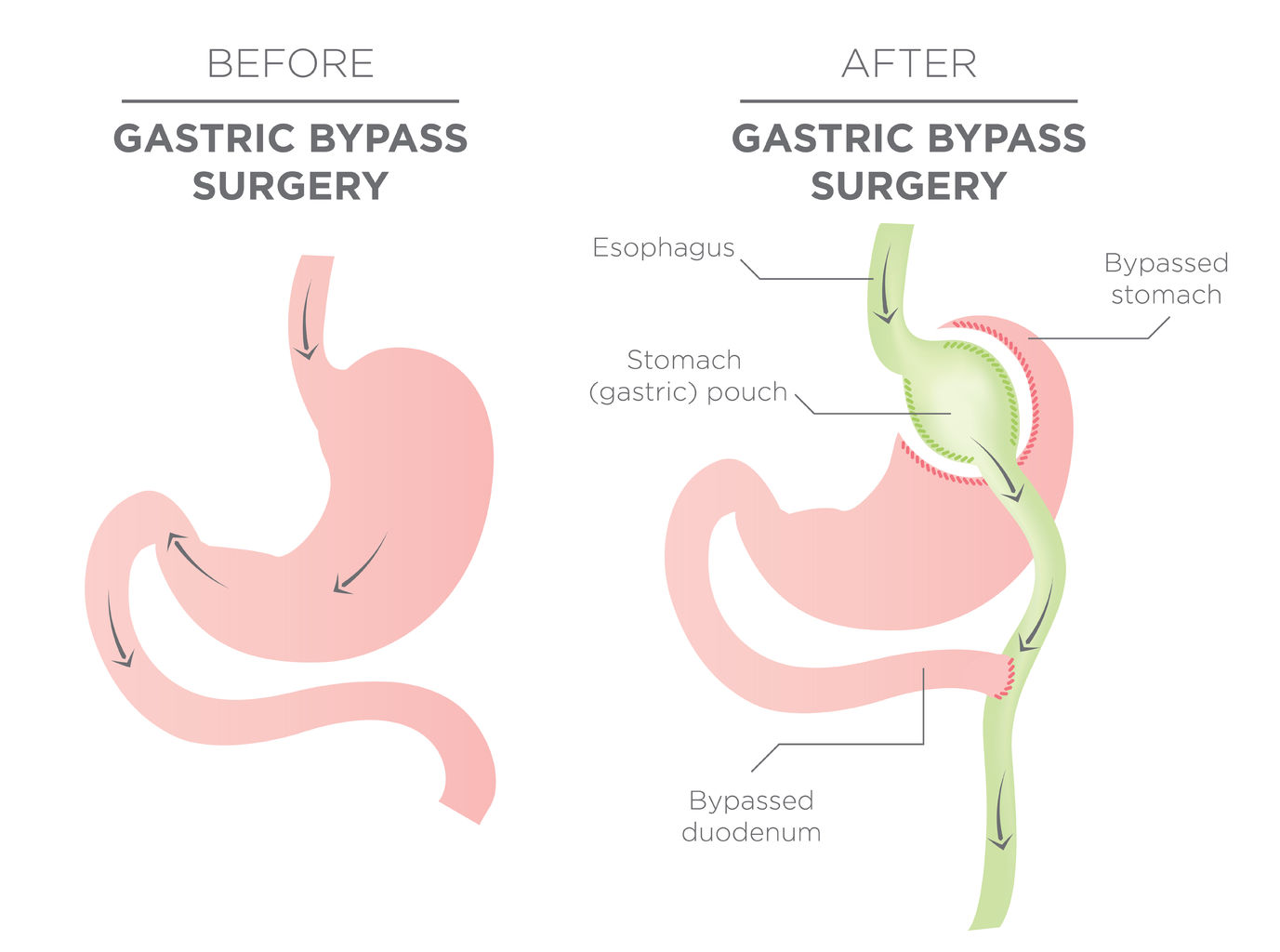
While gastric bypass surgery combines both restrictive and malabsorptive procedures, the other three procedures are all restrictive. Thus, nutritional deficiencies are either absent or minimal after gastric sleeve, Lap-Band or gastric balloon as compared to gastric bypass. In addition, while lap-band and gastric balloon are temporary and do not permanently alter the anatomy of the digestive tract, gastric bypass and, to a minimal extent, gastric sleeve surgeries alter the tract.
Expected weight loss
Weight loss after bariatric surgery depends on many factors apart from the type of surgery itself. These factors are the pre-operative weight of the patient, the competency of the surgeon, the adherence to dietary and exercise plans on the part of the patients, etc. Nevertheless, gastric bypass surgery leads to loss of about 70% of excess weight, followed by gastric sleeve with about 60% of excess weight loss. Lap-Band patients are expected to shed less than 50% of their excess weight. The least is from gastric balloon (32% at 6months reducing to 10.9% at 12months).
Reversal of comorbid conditions
Improvement or total remission of diseases associated with obesity (hypertension, obstructive sleep apnea, diabetes mellitus, osteoarthritis, dyslipidemia, etc.) is the norm after bariatric surgery. This degree of improvement is usually directly proportional to the amount of weight loss. It is therefore not surprising that gastric bypass gives the best result as regard comorbid conditions. This is closely followed by gastric sleeve, Lap-Band and gastric balloon in that order. For example, in a study conducted by Crea et al., type 2 diabetes mellitus incidence reduced from 32.6% to 20.9% while that of hypertension reduced from 44.9% to 30.4% 6months after gastric balloon.1 These are lower when compared to those of gastric sleeve and Lap-Band where resolution in type 2 diabetes were 82.5% and 61.8% respectively.2
Complications
All bariatric surgeries have risks of complications. While complications from malabsorption are extremely rare after gastric sleeve, Lap- Band and gastric balloon, it is a common phenomenon after gastric bypass surgery. the intestinal manipulation that occur during gastric bypass surgery creates some potential spaces where bowel loops can herniate leading to intestinal obstruction, a condition that is almost never seen after Lap-Band or gastric balloon.
Safety
Considering the complication profile, the safest of all is gastric balloon. This is followed by Lap-Band and gastric sleeve surgery respectively. Gastric bypass has the highest risk of morbidity and mortality among these four weight loss procedures.
In conclusion, other surgical weight loss procedures may serve as gastric bypass alternatives. Gastric sleeve, Lap-Band and gastric balloon are relatively safer, cheaper and with fewer complications. However, gastric bypass gives a superior weight loss and reversal comorbid conditions.
References
- Crea N, Pata G, Della Casa D et al. Improvement of Metabolic Syndrome Following Intragastric Balloon: 1 Year Follow-up Analysis. Obesity Surgery. 2009;19(8):1084-1088. doi:10.1007/s11695-009-9879-6.
- Wang S, Li P, Sun XF, Ye NY, Xu ZK, Wang D. Comparison Between Laparoscopic Sleeve Gastrectomy and Laparoscopic Adjustable Gastric Banding for Morbid Obesity: a Meta-analysis. Obesity Surgery. 2013;23(7):980-986. doi:10.1007/s11695-013-0893-3


GLP-1 Delivered
- Lose pounds of fat every week
- Weight Loss Money Back Guarantee
- No membership or hidden fees! Everything you need is included
- Start for just $179, no insurance required + free shipping

TRIMRX - GLP-1 DELIVERED
- 100% online medical review with licensed U.S. providers
- No insurance required
- Transparent pricing
- No hidden fee


